Stroke
Stroke
On This Page
What you need to know about Stroke
A stroke happens when a blood vessel in the brain bursts and bleeds or when the blood supply to the brain is cut off. Blood and oxygen cannot reach the brain’s tissues because of a rupture or obstruction.
Every five minutes, a person suffers a stroke. Every year, 100,000 people experience a stroke. In the UK, there are 1.3 million stroke survivors.
It’s vital to know how to spot the signs of a stroke in yourself or someone else.
A stroke is a medical emergency. The FAST test can help you recognise the most common signs.
- Facial weakness: Can the person smile? Has their mouth or eye drooped?
- Arm weakness: Can the person raise both arms?
- Speech problems: Can the person speak clearly and understand what you say?
- Time to call 999: if you see any of these signs.
Make sure you and your loved ones all know the FAST test.
According to new data from Public Health England, 57,000 people in England experienced their first stroke in 2016. One in six people will have a stroke in their lifetime. About 30% of those who have a stroke will reportedly go on to have another stroke.
Brain tissue and cells are damaged and start to die within minutes of being oxygen-deprived.
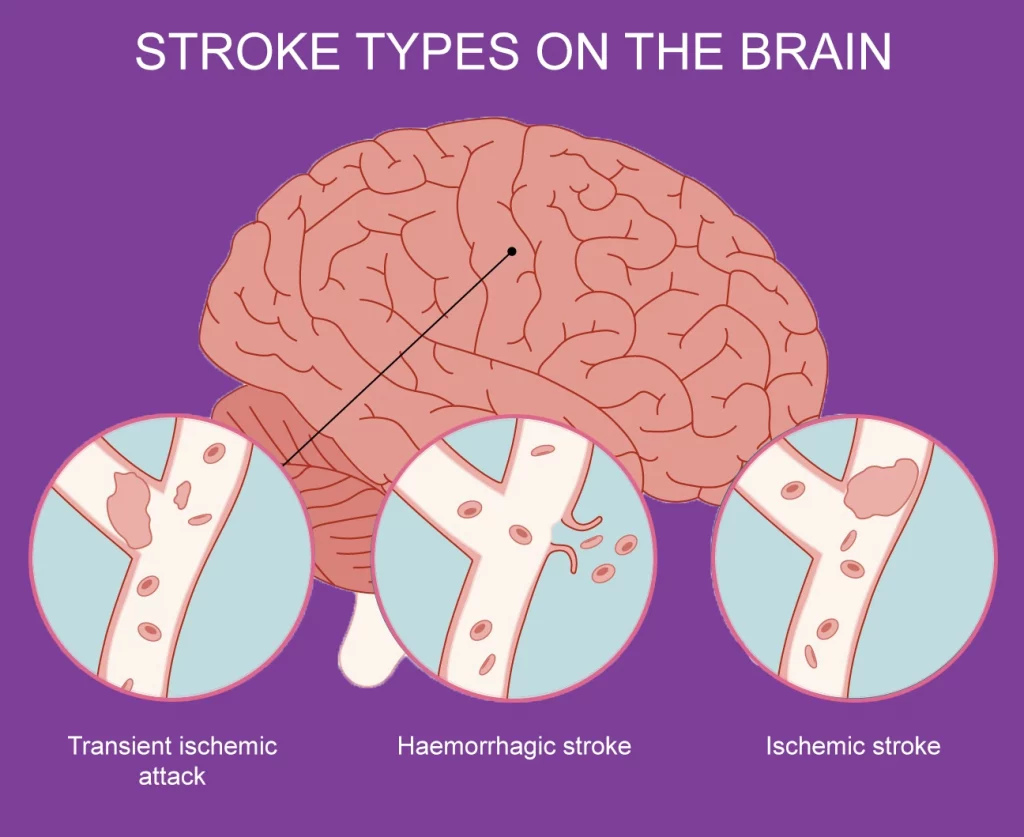
Strokes often come in three different forms:
- Transient ischemic attack (TIA) involves a blood clot that usually dissolves naturally.
- Ischemic stroke involves an arterial obstruction brought on by either a clot or plaque. The signs and problems of an ischemic stroke may persist permanently or linger longer than those of a TIA.
- Hemorrhagic stroke is brought on by a blood artery that leaks or bursts and enters the brain.
Symptoms of Stroke
Damage to brain tissues results from reduced blood supply to the brain. The bodily functions regulated by the brain injury exhibit stroke symptoms.
The better the prognosis for someone experiencing a stroke, the earlier they receive treatment. Because of this, being aware of the symptoms of a stroke will help you take prompt action. Some signs of a stroke include:
- Slurred speech
- Paralysis
- Arm, face, or leg numbness or weakness, especially on one side of the body
- Difficulty communicating or comprehending others
- Lack of response, disorientation, or confusion
- Abrupt alterations in behaviour particularly increased agitation
- Trouble walking
- Issues with one or both eyes’ vision, such as double vision or eyesight that is blurry or blacked out
- Loss of balance or coordination
- Dizziness
- Severe, sudden headache with an unknown cause
- Seizures
- Nausea or vomiting
Any stroke victim needs urgent medical attention. Call 999 or your local emergency services as soon as you suspect that you or someone else is experiencing a stroke. Early intervention is essential to avoiding the following consequences:
- Brain damage
- Long-term disability
- Death
Don’t be afraid to get emergency medical assistance if you believe you have observed the symptoms of a stroke, it’s best to be extra cautious when dealing with a stroke.
Diagnosis
Your doctor will inquire about your symptoms and the circumstances surrounding their onset from you or a close relative. To determine your stroke risk factors, they will review your medical history. Furthermore, they’ll:
- Enquire about the medications you take
- Check your blood pressure
- Listen to your heart
Additionally, you’ll undergo a physical examination, during which your doctor will assess you for:
- Weakness
- Balance
- Coordination
- Arms, face, or legs numbness
- Signs of confusion
- Vision problems
In order to help confirm a stroke diagnosis, your doctor will subsequently perform a few tests. They can use these tests to identify if you had a stroke and, if so, to:
- What may have triggered it
- Which region of the brain is impacted
- Whether you have brain bleeding
Tests to diagnose a stroke
To further assist in determining whether you have had a stroke or to rule out another condition, your doctor may conduct a number of tests. These tests consist of:
Blood tests
For numerous blood tests, your doctor might take a blood sample. A blood test can reveal:
- High blood sugar
- Whether you have an infection
- Platelet counts
- How quickly blood clots
- Cholesterol levels
CT scan and MRI
An MRI scan, CT scan, or both may be prescribed by your doctor.
Any damaged brain tissue or brain cells can be seen with an MRI.
Your brain can be seen in great detail and clarity during a CT scan, which might reveal any bleeding or damage. It can also reveal further brain disorders that could be the source of your symptoms.
EKG
A simple test called an electrocardiogram (EKG) captures the electrical activity of the heart, assessing its rhythm and timing of beats.
An EKG can reveal whether you have any cardiac abnormalities, such as atrial fibrillation or a previous heart attack, that may have contributed to a stroke.
Cerebral angiogram
The arteries in your neck and brain can be seen in great detail in cerebral angiography. Blockages or clots that may have caused symptoms can be shown by the test.
Carotid ultrasound
The carotid arteries, which carry blood to your face, neck, and brain, might have fatty deposits (plaque), which can be seen during a carotid ultrasound, also known as a carotid duplex scan.
Additionally, it might reveal whether your carotid arteries are obstructed or constricted.
Echocardiogram
Your heart’s blood clots can be tracked down with echocardiography. Your brain could have been affected by these clots, leading to a stroke.
What causes a stroke?
The type of stroke will determine the cause. The three primary types of strokes are as follows:
- Transient ischemic attack (TIA)
- Ischemic stroke
- Hemorrhagic stroke
These three groups can be further divided into several stroke types, such as:
- Embolic stroke
- Intracerebral stroke
- Thrombotic stroke
- Subarachnoid stroke
Your treatment options and level of recovery will depend on the type of stroke you experience.
Ischemic stroke
The arteries providing blood to the brain constrict or get blocked during an ischemic stroke. These obstructions are brought either by blood clots or significantly decreased cerebral blood flow. They can also be brought on by plaque fragments that break off and clog a blood artery.
Cerebral thrombosis and embolism are the two obstructions that might cause an ischemic stroke.
When a blood clot forms in another area of the body, usually the heart or arteries in the upper chest and neck, it travels through the bloodstream until it encounters an artery that is too narrow to allow it to pass, which causes a brain embolism (also known as an embolic stroke).
When a blood clot becomes trapped, it prevents blood flow, leading to a stroke.
When a blood clot forms at the fatty plaque inside the blood vessel, cerebral thrombosis, often called thrombotic stroke, occurs.
According to Brain Research UK, Ischaemic strokes account for 85% of all cases. A brain blood vessel burst is what causes hemorrhagic strokes.
Transient ischemic attack (TIA)
A transient ischemic attack, also known as a TIA or ministroke, happens when the brain’s blood supply is momentarily interrupted.
The signs resemble those of a complete stroke. But they usually pass quickly after a few minutes or hours, when the blockage is removed and the blood flow is resumed.
A TIA typically results from a blood clot. A TIA serves as a warning that a true stroke may occur even if it isn’t strictly classified as one. It’s advisable not to ignore it due to this. Get emergency medical aid and seek the same care you would if you were experiencing a massive stroke.
According to Public Health England TIAs are frequently an early warning sign that someone is at risk for a stroke. One in three people who have a TIA go on to have a subsequent stroke within 48 hours following a TIA, there is a very high risk of stroke.
Hemorrhagic stroke
A hemorrhagic stroke occurs when a brain artery bursts or begins to spill blood. The blood from that artery increases the pressure inside the skull and causes the brain to expand, harming the brain’s structures and cells.
The two types of haemorrhagic strokes are Intracerebral and subarachnoid:
- The most frequent kind of hemorrhagic stroke is an intracerebral one. It takes place when an artery ruptures, causing the tissues around the brain to fill with blood.
- Strokes caused by subarachnoid haemorrhage are less frequent. The space between the brain and the tissues that cover it bleeds as a result.
According to the National Institute for Health & Care Excellence (NICE), there are 6–12 cases of subarachnoid haemorrhage per 100,000 persons each year In the UK.
Complications
Complications following a stroke can differ. They could be brought on by either a lasting impairment of abilities or direct harm to the brain during the stroke.
These complications include, among others:
- Cognitive impairment, including dementia
- Seizures
- Loss of bladder and bowel control
- Reduced range of motion, mobility, or capacity to control specific muscle movements
- Depression
- Mood or emotional changes
- Shoulder pain
- Sensory or sensation changes
- Bed sores
These issues can be resolved with techniques like:
- Medication
- Physical therapy
- Counselling
Stroke Risk Factors
You are more prone to stroke if you have certain risk factors. Risk factors for stroke include the following, according to the NHS:
Diet
A poor diet can make you more susceptible to stroke. This kind of diet is high in:
- Cholesterol
- Salt
- Saturated fats
- Trans fats
Inactivity
Lack of exercise or inactivity itself might increase the risk of stroke.
There are several health advantages to regular exercise. Adults should engage in at least 60 minutes of aerobic activity each day, according to the Word Health Organisation (WHO).
Heavy alcohol use
With heavy drinking comes an increased risk of stroke.
If you do drink, do so sparingly. For women, this implies no more than one drink per day, and for men, no more than two drinks per day.
Blood pressure can increase with frequent heavy drinking. Additionally, it may increase triglyceride levels, which may result in atherosclerosis. This is artery plaque buildup, which causes blood vessels to become smaller.
Smoking
Since tobacco use can harm the heart and blood vessels, it also increases the risk of stroke. Blood pressure is also raised by nicotine.
Uncontrollable Risks
You have no control over a number of stroke risk factors, including:
- Family history. Some families have an increased risk of stroke due to inherited health issues including high blood pressure.
- Gender. Strokes can happen to both men and women, but in all age categories, women are more likely to experience them than men.
- Age. The probability of having a stroke increases with age.
- Ethnicity and race. Compared to other racial groups, African Americans, Alaska Natives, and American Indians are more likely to experience a stroke.
Medical History
The risk of stroke is connected to particular medical problems. These consist of:
- Blood clotting disorder
- A previous stroke or TIA
- High blood pressure
- Diabetes
- High cholesterol
- Obesity
- Heart disorders, such as coronary artery disease
- Heart valve defects
- Enlarged heart chambers and irregular heartbeats
- Sickle cell disease
- Patent foramen ovale (PFO)
Speak with your doctor to learn more about your own stroke risk factors.
Treatment
To recover from a stroke, proper medical assessment and timely treatment are essential.
As soon as you suspect a stroke is happening to you or someone else, call 999 or your local emergency services.
Depending on the type of stroke, several treatments are used:
Ischemic stroke and TIA
These different types of stroke are often treated using the same methods because they are all caused by a blood clot or blockage in the brain. They may consist of:
Clot-breaking Medication
Blood clots in your brain’s arteries can be dislodged by thrombolytic medications, which will prevent a stroke and lessen brain damage.
One such medication, tissue plasminogen activator (tPA), also known as Alteplase IV r-tPA, is regarded as the gold standard in the treatment of ischemic stroke.
This medication works by rapidly removing blood clots.
A tPA injection increases recovery from a stroke and decreases the risk of long-term disability in those who receive it.
Mechanical thrombectomy
A catheter is inserted into a large blood vessel inside your head during this surgery by a specialist. The clot is subsequently extracted from the vessel using a device. The optimal window for doing this procedure is between six and twenty-four hours after the stroke starts.
Stents
A technique to expand the constricted artery and reinforce the artery walls with a stent may be used if a doctor discovers areas where the artery walls have weakened.
Surgery
Surgery can be used to remove a blood clot and artery plaques in the uncommon event that other therapies fail.
A catheter might be used during this procedure. An artery may need to be opened by a surgeon if the clot is particularly large in order to be removed.
Hemorrhagic stroke
Different approaches to treatment are necessary for strokes brought on by bleeding or leaks in the brain. Hemorrhagic stroke is treated with:
Medications
In contrast to an ischemic stroke, the goal of treatment for a hemorrhagic stroke is to induce a blood clot. As a result, you can be prescribed medication to balance out any blood thinners you take.
Additionally, medications that can:
- Lower blood pressure
- Reduce the pressure in your brain
- Seizures prevention
- Prevent constriction of the blood vessel
Coiling
Your doctor performs this treatment by directing a long catheter to the bleeding or blood vessel weakness. The weak spot in the artery wall is then treated with a coil-like device. This lessens bleeding by obstructing blood flow to the location.
Clamping
Your doctor may find an aneurysm during imaging exams that has either not yet started bleeding or has stopped.
A surgeon could insert a tiny clip at the aneurysm’s base to stop further bleeding. This stops the flow of blood and stops any potential bleeding or new blood vessels from breaking.
Surgery
When an aneurysm bursts, your doctor may perform surgery to clip the aneurysm and stop further bleeding. Similar to how a big stroke may necessitate a craniotomy to release pressure on the brain.
Your medical team will provide you with emergency care as well as stroke prevention tips.
Medication for stroke
Strokes can be treated with a variety of medications. The kind of stroke you suffered has a significant impact on the medication your doctor will prescribe.
Some drugs work to stop a stroke from happening again, while others try to stop a stroke from occurring in the first place.
Depending on factors including your medical history and risk factors, your doctor may recommend one or more of these drugs to treat or prevent a stroke.
The most often used stroke treatments include:
Anticoagulants
These medications lessen your blood’s capacity to clot. Warfarin is the most often used anticoagulant (Coumadin, Jantoven).
These medications may be prescribed by doctors to prevent a stroke or after an ischemic stroke or transient ischemic attack (TIA) because they can stop blood clots from getting larger.
Antiplatelet medications
These drugs work to prevent blood clots by making it more difficult for platelets in the blood to adhere to one another. The two most widely used antiplatelet medications are aspirin and clopidogrel (Plavix).
The medications can stop ischemic strokes. They’re crucial in preventing subsequent strokes, in particular.
Aspirin should only be taken as a preventive measure if you have a high risk of atherosclerotic cardiovascular disease (such as heart attack and stroke) and a low risk of bleeding if you’ve never had a stroke before.
Direct-acting oral anticoagulants (DOACs)
This more recent medicine class reduces your blood’s capacity to clot in the same manner as traditional anticoagulants do, but it frequently acts more quickly and with less oversight.
DOACs have the potential to lower the risk of brain bleeding when used to prevent stroke.
Statins
By lowering high blood cholesterol levels, statins aid. They rank among the most frequently prescribed drugs in the US.
These medications stop the synthesis of an enzyme that can transform cholesterol into plaque, the fatty, gooey substance that can clog arteries and result in heart attacks and strokes.
Typical statins consist of:
- Atorvastatin (Lipitor)
- Rosuvastatin (Crestor)
- Simvastatin (Zocor)
Tissue plasminogen activator (tPA)
To dissolve the blood clot that is during a stroke, this emergency medication might be administered. It must be administered between three and four hours after the onset of stroke symptoms because it is the only medicine on the market that can accomplish this.
In order for the treatment to begin working as soon as possible and lower the chance of consequences from the stroke, this substance is injected into a blood vessel.
Blood pressure medications
Broken bits of plaque buildup in your arteries may result from high blood pressure. These fragments may obstruct arteries and result in a stroke.
Therefore, controlling high blood pressure with medication, a change in lifestyle, or both can aid in preventing a stroke.
In the UK, stroke is one of the main causes of long-term impairment.
However, according to the Stroke Association, 10% of stroke survivors recover virtually completely, while another 25% only experience minor problems.
After a stroke, it’s critical to begin recovery and rehabilitation as soon as possible. Recovery from a stroke should actually start in the hospital.
In a hospital, a medical team can assess the stroke’s consequences and stabilise your condition. They can pinpoint the underlying causes and start therapy to aid you in regaining some of your lost abilities.
Four primary areas are often the focus of stroke recovery:
Cognitive therapy
Many people may have changes in their ability to think and reason after a stroke. Changes in mood and behaviour may result from this.
You can manage your emotional responses and strive to reestablish your previous thought and behaviour patterns with the assistance of an occupational therapist.
Physical therapy
After a stroke, your muscle tone and strength may diminish, making it difficult to move your body as well as you once could.
Your strength and balance will be restored, and a physical therapist will help you find ways to work around any restrictions.
You can receive rehabilitation in your home, a skilled nursing facility, or a clinic.
Relearning sensory skills
Your senses may become “dull” or cease to function if the area of your brain that sends sensory data is damaged during the stroke.
This could indicate that you have poor sensation for things like pain, pressure, or temperature. You can learn to get used to this absence of sensation with the assistance of an occupational therapist.
Speech therapy
Speech and language difficulties can be brought on by a stroke. You will work with a speech and language therapist to relearn how to talk.
They can also assist you in finding alternative forms of communication if verbal interaction is challenging for you after a stroke.
Outlook
You must get emergency medical care as soon as you can if you think you could be having a stroke.
Only in the first few hours following the onset of stroke symptoms can clot-busting therapy be given. One of the best methods to lower your chance of long-term problems and disability is to seek treatment as soon as possible.
Even though a stroke cannot always be avoided, making some lifestyle modifications can significantly lower your risk. The danger of blood clots, which can result in stroke, can also be decreased with the aid of medications.
Your doctor will work with you to develop a preventative plan that is effective for you if they suspect you may be at risk of having a stroke. This plan may include medication intervention as well as dietary and lifestyle adjustments.